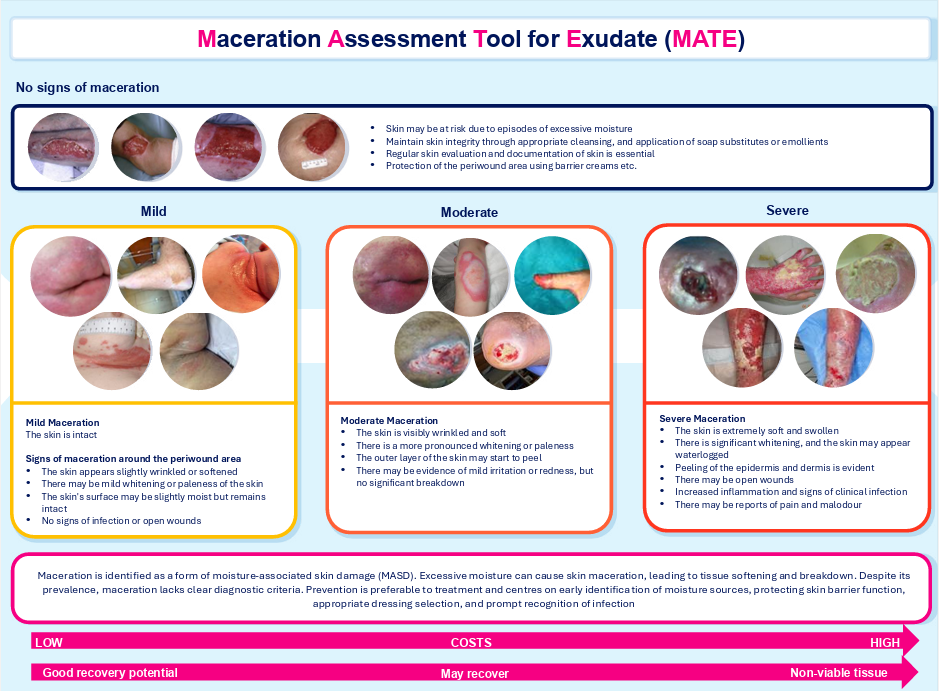
Debridement: an overview
Debridement is ‘the removal of nonviable tissue, including necrotic material, slough, microorganisms, biofilm and contaminants from or adjacent to a wound’ (International Wound Infection Institute [IWII], 2022).
Non-viable tissue often presents in acute wounds (e.g. surgical wounds/skin tears) and chronic wounds (e.g. DFUs [Image 1]; venous leg ulcers [VLUs]; pressure ulcers [PUs] and ischaemic ulcers [Percival and Suleman, 2015]. Chronic wounds (Image 2 a-d) are more likely to require debridement than others, as they are more likely to contain non-viable tissue and slough that harbour microorganisms and increase the risk of infection (Nair et al, 2022).
Non-viable tissue creates an abnormal wound environment that interferes with the healing process (Vowden and Vowden, 2011) and serves as a source of nutrients for bacteria (Manna et al, 2023), promoting microbial proliferation and biofilm formation, whilst reducing the effectiveness of topical antibiotics and antiseptics (Anghel et al, 2016; IWII, 2023). While removing non-viable tissue, debridement also reduces biofilm and stabilises the microbiome of the periwound skin, creating a good environment for healing and reducing the risk of infection (Young et al, 2013; Sen et al, 2021; Thomas et al, 2021). An integrated, collaborative interdisciplinary approach is required when making decisions regarding debridement; therefore, debridement is an important step in infection prevention, management and biofilm removal (IWII, 2022).
Wound bed preparation
Wound bed preparation (WBP) is a framework for the assessment, diagnosis and treatment of wounds. It involves therapeutic wound cleansing, debridement and the prevention of biofilm reformation (Haubner et al, 2012).
TIMERS (Atkin et al, 2019) is a recommended framework which provides an extension of the original TIME framework incorporating 6 elements of WBP:
- Tissue
- Inflammation/infection
- Moisture balance
- Edge of wound/Epithelialisation
- Repair and regeneration
- Social factors.
The aim of WBP is to create a balanced, moist environment, optimising conditions for debridement and wound healing, producing a well-vascularised, stable wound bed to reduce microbial load, manage exudate levels and increase granulation tissue formation (Schofield and Ousey, 2021; Barrigah-Benissan et al, 2022). Debridement and cleansing are essential to wound healing, and it is important to distinguish between the two.
Cleansing
Effective cleansing is important to optimise debridement. Wounds should be cleansed before and after debridement. Cleansing improves the visibility of the wound bed, facilitates accurate assessment and allows access to non-viable tissue, yet it is not the comprehensive removal of devitalised tissue (that is the role of debridement; IWII, 2022). Acidic cleansers, such as hypochlorous acidic cleansers, can soften slough and thus optimise the debridement process.
The purpose of cleansing is to reduce the bioburden, including bacteria, debris and contaminants and remove any loose material (e.g. dried blood, dressing residue and eliminate wound exudate; IWII, 2022). Cleansing can also support the removal of slough and necrotic tissue (Olszowski et al, 2003; Pattison et al, 2003; Brown,2018).
Several types of solutions can be used for cleansing, including tap water, saline, povidone-iodine and agents containing antimicrobials and/or active preservatives (e.g. hypochlorous acid [HOCI], sodium hypochlorite, octenidine dihydrochloride and polyhexamethylene biguanide [PHMB]). There is no specific recommended wound cleansing solution, as choice depends on wound assessment (e.g. aetiology, and anatomical location), risk of wound infection, goals of care and local policies and resources (IWII, 2022). Cleansing solution must remain in contact with the wound bed for the recommended time to achieve optimum cleansing (Nair et al, 2023).
Although each solution offers distinct benefits and carries various risks, as a naturally occurring molecule with a high therapeutic index, it is established that HOCI does not harm healthy tissue or cause a stinging sensation, making it suitable for frequent application (Mayer et al, 2024).
Debridement use and techniques
Following cleansing, clinicians should consider the following questions when selecting the most appropriate method of debridement (adapted from Vowden and Vowden, 2011):
- What is wound aetiology?
- Where is it anatomically located?
- How much non-viable tissue needs to be removed?
- What is the aim of treatment?
- What are the risks and benefits of the proposed debridement method?
- What speed of debridement is required?
- Which method would be most appropriate?
- Are the necessary skills and/or equipment required to perform optimal debridement available in the practice/care setting?
Debridement: Who should do it?
Debridement is an essential step in wound healing, which is underused in practice, possibly due to a lack of clinician knowledge, practice and sometimes confidence for some options/procedures that could be appropriate. Decisions to debride are often complex and may require input from a multidisciplinary team.
Clinicians should have appropriate training and be competent in the techniques used, in accordance with local policy. Once the decision to proceed with debridement and the preferred method has been determined, clinicians must assess their skills and competency to undertake the process.
Competent clinicians performing wound debridement are expected to have the following skills (Vowden and Vowden, 2011):
- Good knowledge of relevant anatomy
- Understanding of the range of wound debridement methods available
- Capability to identify viable tissue and differentiate it from non-viable tissue
- Ability to manage pain and discomfort before, during and after the procedure
- Appropriate skills to handle potential complications (e.g. bleeding)
- Awareness of infection control procedures.
Debridement: frequency
A single session of debridement may be sufficient for some wounds, others need repeated (continuous) sessions to clean those wounds and to prevent them from reverting to a chronic unhealthy state, as devitalised tissue can often resurface due to underlying causes. These wounds need to be monitored at every clinical visit, a practice known as maintenance debridement (EWMA, 2004; Jones, 2018; Thomas et al, 2021).
Debridement: Patient selection and preference
It is important to engage the patient in their care and the decision-making process so that they understand the options and make informed decisions about their care. Clinicians have a legal responsibility to explain all available debridement methods and potential outcomes – e.g. reducing the risk of infection/the possibility of the wound getting larger in size (Haycocks and Chadwick, 2012) and ensure that patients understand. In some types of debridement, informed consent must be formally obtained; refer to local policy where necessary,
Infection risk
Infection is a common and serious complication and can develop in any wound, clinicians must be skilled in recognising and assessing signs of wound infection e.g. purulent discharge, erythema, swelling, localised warmth, malodour, and new or increasing pain (IWII, 2022). It should be noted that some wounds are at a higher risk of infection than others (DFUs are at particularly high risk), or patients may be at higher risk (due to factors such as comorbidities or immunosuppression) and may need particular vigilance.
In immunocompromised individuals and those with chronic wounds, infection may present with subtle or covert signs, which require careful observation (IWII, 2022). Signs of wound infection to consider include overt symptoms, such as (IWII, 2022):
Erythema (which may present differently depending on the individual’s skin tone) may include:
- Local warmth
- Swelling
- Purulent discharge
- Wound breakdown and enlargement
- New or increasing pain
- Increasing malodour.
More covert or subtle symptoms may also occur, such as (IWII, 2022):
- Friable, bright red granulation tissue
- Increased malodour
- New increased pain or change in sensation
- Epithelial bridging and pocketing in granulation tissue
- Delayed wound healing beyond expectations
- Wound breakdown and enlargement or new ulcerations of the periwound.
Pain
Pain can be an indicator of ineffective wound management where the underlying causal pathology has not been identified or treated, or infection is present (Price et al, 2008). Pain can impact every aspect of an individual (e.g. quality of life, ability to function, social and psychological wellbeing; Holloway et al, 2024).
Pain management may be required as part of the debridement process itself, and the patient must be as prepared as possible for the procedure and aware of what to expect (WUWHS, 2016). Studies have shown that following the updated non-cancer pain ladder can improve patient outcomes and quality of life, as well as reduce hospital stays (Guiloff and Angus-Leppan, 2016; Anekar et al, 2023).
Focus on autolytic debridement
Autolytic debridement is generally considered as the most conservative debridement method, which can be facilitated by clinicians in any care setting following a full holistic assessment. This type of debridement is a natural process by which the body’s own enzymes break down necrotic tissue, inducing softening of the necrotic tissue and detachment of this tissue from the wound bed (IWII, 2022). It is a highly selective process whereby only necrotic tissue will be affected (Manna et al, 2023).
When needed, autolytic continuous debridement can be used in conjunction with other debridement techniques (e.g. mechanical/sharp debridement) as part of an ongoing care pathway (Vowden and Vowden, 2011). This can be facilitated using various wound dressings, such as polyabsorbent fibres, fibre-gelling, as well as hydrofibre, alginate, hydrogel, hydrocolloid and transparent film, dressings that promote autolysis of necrotic tissue (Sibbald et al, 2021; IWII, 2023). This requires maintaining a balanced moist environment, achieved with either moisture-retentive/moisture-donating dressings, depending on the wound; effectiveness is influenced by the amount of devitalised tissue and the size of the wound (Manna et al, 2023).
Autolytic continuous debridement can be performed using specific dressings, such as polyabsorbent fibre dressings. These dressings may or may not be impregnated with silver salts, depending on the wound’s status, including any local signs or risk of infection. Dressings made of polyabsorbent fibres have demonstrated continuous debridement on slough removal (Dissemond et al, 2020a, 2020b; Meaume et al, 2014), facilitated by their high negative charge (Desroche et al, 2016).
Link to biofilm management
Management of biofilm is acknowledged as a primary aim of wound care, particularly in chronic wounds. Biofilms are aggregates of microorganisms that attach to biotic (living surfaces, e.g. biological tissues), abiotic surfaces (non-living surfaces, e.g. wound dressings) or each other.
Studies suggest that between 60% and 100% of chronic wounds contain biofilm, with the ‘true’ prevalence likely approaching 100%, indicating that all chronic wounds may have biofilm on at least part of the wound bed (Bjarnsholt et al, 2017; Malone et al, 2017). Biofilms are not visible to the naked eye, but downstream effects can provide some clinical cues.
Effective management involves employing antibiofilm therapies and strategies to remove or disrupt both the microorganisms and the extracellular polymeric substance. This helps reduce microbial reattachment and prevents biofilm reformation.
Use of polyabsorbent fibre dressings impregnated with silver salts through a TLC-Ag matrix, which offer autolytic continuous debridement and antimicrobial properties, have been found to be a beneficial option in biofilm-based wound care, being effective against bacteria such as Staphylococcus aureus, MRSA, Streptococcus pyogenes and Pseudomonas aeruginosa (Desroche et al, 2016).
Pathway for biofilm management
Debridement must be viewed as part of a wider care pathway for wound management, following a holistic assessment and setting priorities and treatment goals in collaboration with the patient. This should encompass all the needs of the patient and their wound, according to a structured protocol such as T.I.M.E.R.S (Atkin et al, 2019) or local protocol.
Pathway for use in practice
The Pathway for Biofilm Management (provides a checklist for each stage to support clinicians in selecting autolytic debridement for wounds, particularly those that are chronic and may include biofilm.
Access the full consensus document here.