1. The gut biome is just beginning to be understood and appreciated
Healthcare providers know about the “bacterial load” in faeces, but the numbers are impressive. The human intestine harbours more than 100 trillion bacteria with Bacteroidetes and Firmicutes as the most abundant phylotypes. Maintaining the gut biome is important to immune health and when altered, the biome contributes to many other diseases than just gastrointestinal disease, such as allergies, heart disease and multiple sclerosis to name a few.
2. Antibiotics decimate bacteria in the gut
Sepsis is a leading cause of admission to intensive care units (ICUs) worldwide, accounting for more than 30% of all admissions. The morbidity and mortality for septic patients in ICUs is >50%. (La Via et al, 2025). The management of sepsis is time-sensitive, and the timely initiation of effective antimicrobial therapy is one of the strongest predictors of survival. Combinations of antibiotics are given until the specific organisms are known. Therein lies the risk-benefit ratio. Antibiotics are crucial, but act like a “wildfire” in the gut, indiscriminately killing beneficial bacteria, such as Bifidobacterium and Lactobacillus, alongside pathogens (Peltak and Steen, 2025).
3. Faecal injury to skin has many causes
Some of the causes of injury to the skin may be obvious. A multivariate analysis by Deprez et al, 2024 outlined the risk ratios . Antibiotic use increased the odds of skin injury by 2.72 to 3.16. Having more than three episodes of loose stool increased the risk of skin injury 21.98 times. Loose or liquid stool had an odds ratio for skin injury ranging from 20.61 to 51.05. However, there were less obvious risks, including vasopressor use (odds ratio 19.44). Female gender and older age also increased risk.
4. Tube feeding protocols may be part of the problem
Tube feeding patients with crucial illness is an unphysiological way of administering nutrients. Critical illness is a state of anabolic resistance and the time point when an adequate response to feeding does occur cannot be predicted or reliably monitored. However, tube feeding has been long considered the only way to feed the critically ill patient. When tube feeding is provided in very small volumes, the usual postprandial physiology is not stimulated. Normal postprandial physiology requires a fairly substantial caloric load at least 530 kcal as a bolus being required (Bowling, 2010). Despite this long-established knowledge, most patients are still given “trophic rates” of 20–50 ml per hour. More research is needed to identify the most beneficial method to maintain the gut health and prevent dysbiosis, where beneficial bacteria are lost and opportunist ones thrive.
5. Antibiotic-associated diarrhoea is not an innocuous problem
Three or more antibiotics or antibiotics combined with antifungals increases the incidence of antibiotic-associated diarrhoea to 44% (Ma et al, 2019). A large systematic review of more than 13,000 patients reported that diarrhoea was associated with an increased relative risk of ICU mortality (RR 1.43), greater lengths of ICU stay (RR 8.08) and longer total hospital stay (RR 9.67) (Taito et al, 2019).
6. Clostridodes difficile has a new name, but remains a serious problem
The genus name changed from Clostridium in 2016 when molecular sequencing was performed; however, it is still known as “C diff” in clinical work. C difficile develops when the gut biome is out of balance especially from vancomycin, clindamycin, fluoroquinolones and cephalosporins. Pathogenic C difficile strains produce multiple toxins: an enterotoxin (C difficile toxin A) and cytotoxin (C difficile toxin B), both of which may produce diarrhoea and inflammation in infected patients. C difficile colitis can be treated with fidaxomicin, faecal transplant and sometimes requires colectomy with end ileostomy (Pumiglia et al, 2024).
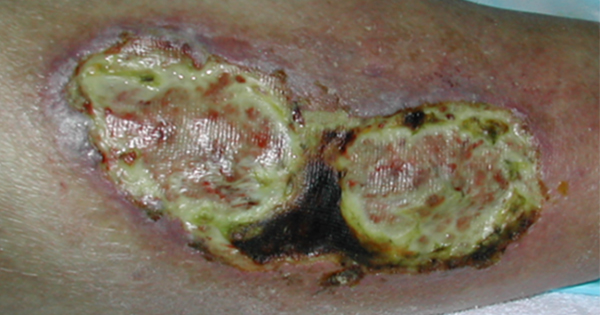
7. Do not use soap and water on injured skin
Skin damaged from diarrhoea is open and inflamed [Figure 1]. Do not clean the skin with soap and water. Soap is often alkaline and will further injure the skin. Use pH balanced liquid soap on soft cloths without scrubbing. Chlorhexidine, commonly used on intact skin, cannot be used on open skin or mucous membranes. Hypochlorous acid can be used to reduce the bacterial load on the skin. It should be left on the skin for 5 minutes.
8. Contain the liquid stool
Over the years many products have been used to collect liquid stools, including nasal trumpets and urinary catheters. Those products were reported to lead to necrosis of the rectum and have been largely discontinued. Adhesive pouches can be applied, but do carry the risk of skin damage when removed. A soft, silicone catheter inserted into the rectum, with an inflatable balloon to hold it in place and a collection bag to contain the waste is the most effective method. These devices provide an effective closed system for managing faecal incontinence, minimising skin breakdown, protecting against infection, and reducing caregiver burden.
9. Educate the ICU staff on how to use faecal containment systems
While diarrhoea is common in critically ill patients, not all staff will be familiar with methods to contain liquid stool. Generally, it is wise not to wait until there is skin damage. It is not easy to insert a balloon into a patient with frequent diarrhoea or incontinence. Therefore, staff need to develop proficiency in the use of faecal management systems. Contraindications to use include increased risk of bleeding (due to anticoagulation or clotting disorders), severe haemorrhoids, rectal tumours or strictures, or recent colorectal surgery.
Once in place, the device needs to be monitored for leakage, kinks in the tubing, and to ensure gravity flow of stool. The faecal management system tubing should be placed so there are no kinks or taut tubing. Flushing the system can help maintain patency and reduce odour. The skin around the device should be inspected for damage from straps or adhesives.
10. Moisturise the cleansed skin and protect the skin with a barrier product
Once the skin is cleaned, it needs to be moisturised to promote healing, and a barrier should be applied to reduce exposure from the next bout of diarrhoea. Faecal incontinence is a major risk factor for pressure ulcer development.
Faecal incontinence is not a complication of critical illness that should be taken lightly. Serious injury can occur to the skin and lead to pain and pressure ulcers.