We will organise the ten top tips into ten top medication classes and explain how each medication class works and how it impairs wound healing (Beitz 2017; Khalil et al, 2017).
1 – Anticoagulants are commonly used and alter early healing
Examples: rivaroxaban and warfarin.
Anticoagulants are frequently used to prevent development or worsening of venous thromboembolism, reducing emboli in atrial fibrillation and preventing occlusion of percutaneous coronary intervention stents. The mechanism of action of anticoagulants varies between drug classes, but the common underlying outcome is interruption of the clotting cascade, resulting in prolonged bleeding time (Umerah and Momodu, 2023).
When treating patients with chronic wounds who are on anticoagulants, it is essential to understand that the wound healing phases can be affected during the inflammatory phase. In the initial hours after a wound occurs (inflammatory phase) and without interference of the anticoagulant, the body’s normal reaction to a wound is the release of adenosine 5’ diphosphate (ADP), followed by the blood platelets clumping and the beginning of thrombosis. However, anticoagulant medications prevent clot formation and lead the individual to develop a hard-to-heal wound.
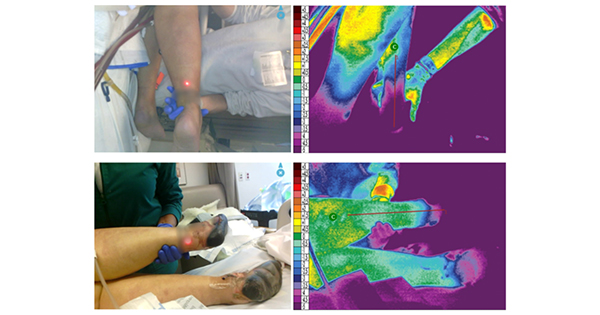
In addition, one of the wound healing complications caused by anticoagulants is skin necrosis, which can occur when using heparin or warfarin. This condition leads to painful lesions on the skin that may occur in the thighs, abdomen or breasts. Skin necrosis appears commonly in areas of trauma [Figure 1].
2 – Nicotine is a powerful vasoconstrictor
Examples: cigarettes, vapes, cigars, second-hand smoke.
It has been estimated that cigarette smoke contains more than 4,000 toxic compounds. The primary toxins associated with impaired wound healing are nicotine and carbon monoxide and hydrogen cyanide gases. The definitive mechanisms through delay healing are not understood, but all have been shown to impair oxygen supply to tissues (McDaniel and Browning, 2017).
Nicotine is known to cause tissue hypoxia. Nicotine is a colourless alkaloid that is rapidly absorbed during smoking; it is hypothesised that it acts as a major component of reduced blood flow due to its vasoconstrictive actions. Some studies suggest that nicotine is harmful to skin and subcutaneous tissue because it stimulates the sympathetic nervous system to release catecholamines, which trigger peripheral vasoconstriction and diminish tissue perfusion rates.
Patients should be counselled on the risk of continuing to smoke, including decreased blood flow and oxygen to wound, increased risk of infection, slower healing, and decreased strength of scar tissue.
A study of patients having plastic surgery reported that nicotine replacement therapy carried similar risks as continued smoking and is not as safe as abstinence in the perioperative period.
Importantly, patients who stopped smoking for surgery had an equivalent risk for postoperative complications as patients who had never smoked (Michaels et al, 2018).
3 – Expect significant delays in healing if anti-inflammatory medications are in use
The first six medication classes outlined below all impair the inflammatory phase of wound healing.
The inflammatory response is often considered the major aspect of healing, and it has been said that when there is no inflammation, there is no healing. The inflammatory process is an immediate reaction to the foreign protein on bacteria, damaged cells from trauma and many other causes. The body uses inflammation in response to many conditions. In wounds, inflammation protects from further damage from the antigen. Histamine, bradykinin, and prostaglandins are released which open the capillary bed, produce oedema, and isolate the antigen so it can be phagocytised by leukocytes.
Sometimes inflammation must be controlled to reduce damaging oedema; however, the wound healing will slow. The inflammatory cascade also prompts the remaining three phases of healing, so the impact is long lasting.
4 – Corticosteroids are the most common anti-inflammatory seen in clinical practice
Examples: prednisone and methylprednisolone.
The mechanism of action of corticosteroids is complex. These medications are synthetic versions of cortisol, which is responsible for numerous activities in the body, including mediating the stress response, the inflammatory response, immune function and metabolism (Thau et al, 2023). Corticosteroids interfer with inflammation, fibroblast proliferation, collagen synthesis and degradation, deposition of connective tissue ground substances, angiogenesis, wound contraction and re-epithelialisation. These actions occur through antagonism of various growth factors and cytokines.
As stated previously, delaying, prolonging, or reducing the inflammatory phase of healing will have long-lasting effects on wound healing, regardless of the wound type.
5 – Non-steroidal anti-inflammatory drugs (NSAIDs) significantly impair bone healing
Examples: ibuprofen and ketorolac.
NSAIDs are among the most frequently used and prescribed medications in the management of musculoskeletal pain and injury. However, there is evidence to suggest that long-term use of NSAIDs for managing fracture pain and inflammation carries the risk of impaired bone healing. Many providers add these medications to promote multimodal pain management and reduce the dependence on opiates.
NSAIDs inhibit the enzyme cyclooxygenase (COX), which is required to convert arachidonic acid into prostaglandins, thromboxanes, and prostacyclins (Ghlichloo and Gerriets, 2023). In addition, the adverse effects of NSAIDs on the gastrointestinal, renal and cardiovascular systems are serious.
The introduction of cyclooxygenase (COX)-2 inhibitors, or coxibs, held the promise of providing the same therapeutic benefits as nonspecific NSAIDs with fewer gastrointestinal adverse effects. However, this class of medications has been shown to have potentially serious consequences for the cardiovascular system.
6 – Anti-rejection/immunosuppressant medications negatively influence the wound-healing process
Examples: tacrolimus and cyclosporine.
Several inflammatory mediators involved in the wound-healing process are affected by immunosuppressants. Anti-rejection medications suppress the T lymphocytes, targeting T-helper cells and T-suppressor cells. These cells play a vital role in wound healing, especially in the inflammatory phase. Depletion of CD4+ T cells (helper T cells) results in decreased wound tensile strength.
Cyclosporine A (CsA) is a cyclic peptide of fungal origin that inhibits T-cell response and calcineurin. When calcineurin is inhibited, cytokine genes (IL-2, IFN‐γ, GM-CSF, TNF‐α and IL-4) cannot be transcribed. This cascade of events ultimately results in inhibition of T‐cell production and differentiation.
Tacrolimus is a product of the fungus Streptomyces tsukubaenis. It is a calcineurin inhibitor and is potent in delaying healing, by 10–100-fold more than CsA . Tacrolimus also decreases nitric oxide synthesis which impairs wound healing. The inhibition of T‐cell proliferation brought about by either CsA or tacrolimus can be partially reversed by the addition of exogenous interleukin-2 to in vitro culture.
Stopping an immunosuppressant medication to allow for wound healing may be a reasonable choice but must be a shared decision for each individual patient (Tapia et al, 2023).
7 – Immunomodulators increase the risk of serious infections
Examples: infliximab, etanercept.
Biologic response modifiers or immunomodulators are used in autoimmune diseases as first-line medications or after the failure of conventional agents. Serious infections are the most feared complications and require screening before initiation and monitoring while patients are taking the medications. Unusual infections, including mycobacteria (leprosy and non-tuberculous mycobacteria) and infections from mould and fungi have been reported.
Despite the perceived challenge of treating chronic wounds in immunocompromised patients, there is a lack of clinical guidelines that can help wound care specialists and podiatrists provide a structured treatment. Clinicians need to rely on their clinical judgment to make the best treatment choice for their patients.
The clinical signs and symptoms of wound infection might be less apparent in immunocompromised patients. Therefore, clinicians should obtain regular wound cultures and monitor the antimicrobial sensitivity profiles of these patients. This practice will allow wound care specialists to provide empirical antibiotic therapy that is tailored to the wound culture results (Bootun, 2013).
8 – Tumour necrosis factor (TNF) controls many aspects of wound healing
Examples: adalimumab and golimumab.
TNF promotes the inflammatory activity of macrophages and also controls macrophage survival and death. TNF exerts its activities by stimulation of two different types of receptors, TNF receptor-1 (TNFR1) and TNFR2. The mechanism of action for TNF inhibitors is to block the binding of TNF to its receptors preventing the inflammatory and immune response. In order for cells to growth and reproduce, oxygen and nutrients are needed.
New vessels form from existing vessels, called angiogenesis. Angiogenesis is stimulated by inflammatory cells. Thus, inflammation and the following angiogenesis are tightly connected. In addition, TNF-α regulates the activity of fibroblasts, vascular endothelial cells and keratinocytes, and the synthesis of extracellular matrix proteins and matrix metalloproteinases, which are closely involved in the healing of injured tissues.
TNF inhibitors are often used in the treatment of autoimmune diseases. Notably, golimumab is used for the treatment of inflammatory bowel disease, in which pyoderma gangrenosa can occur (Sadiq et al, 2023).
9 – Colchicine reduces inflammation and collagen deposition
Colchicine is commonly used for the treatment of gout. It is an anti-inflammatory and inhibits activation, degranulation, and migration of neutrophils associated with gout symptoms. Sometimes, colchicine is used as a component of multimodal pain relief.
Despite its positive outcomes in pain reduction, colchicine decreases wound healing though suppression of neutrophil and subsequent proinflammatory macrophage infiltration around the wound site.
Furthermore, colchicine significantly reduces the breaking strength of wound scar tissue due to lowered collagen synthesis (Gerriets et al, 2023).
10 – Chemotherapeutic medications inhibit cell proliferation
Examples: doxorubicin and cyclophosphamide.
Doxorubicin, cyclophosphamide and other agents used for chemotherapy are developed to prevent cell proliferation to reduce the tumour development due to excessive uncontrolled cell growth.
When a wound is in the proliferative phase, these medications will hamper new cell growth, as that is what they are designed to do.
Like the other medications previously discussed, the effects on cell growth are not specific to the cancer; they affect every dividing cell.
Chemotherapy medications can also cause wounds, especially when given peripherally, and can cause extravasation.
Additionally, white blood cells are rapidly growing cells and are wiped out by chemotherapy, therefore, increasing the risk of infection from the open wound. It is crucial the patient and caregivers are educated to cleanse the wound appropriately with an antimicrobial cleanser and maintain clean wound dressings, ideally with an antimicrobial dressing, to reduce the risk of infection (Amjad et al, 2023).
Conclusion
As with all medications, a comprehensive medication reconciliation is crucial for appropriate care. After reviewing the medication list, apart from nicotine, it is unlikely that the patient can stop taking these previously discussed medications.
The patient and family should be taught that healing will be slow and, therefore, the risk of infection will be high.