While chronic wounds have devastating consequences for patients and contribute significant costs to health care systems and society, health care professionals (HCPs) find assessing, treating and healing chronic wounds a challenge (Posnett and Franks, 2008; Patel et al, 2008; Frykberg and Banks, 2015; Guest et al, 2015, 2020; Olsson et al, 2019; Martinengo et al, 2019; Keast et al, 2020). In their 2019 study, Keilo et al concluded that healthcare providers who manage a variety of wounds require standardised treatment and referral guidance to effectively treat wounds within a multidisciplinary environment (Keilo et al, 2019). HCPs report the difficulties they experience are due to the prevalence of ritualistic practice, lack of overall wound-care knowledge, the fragmented linkages between evidence and practice and in the lack of structured wound-care education (Welsh, 2018; Keilo et al, 2019; Tayyib and Ramaiah, 2021).
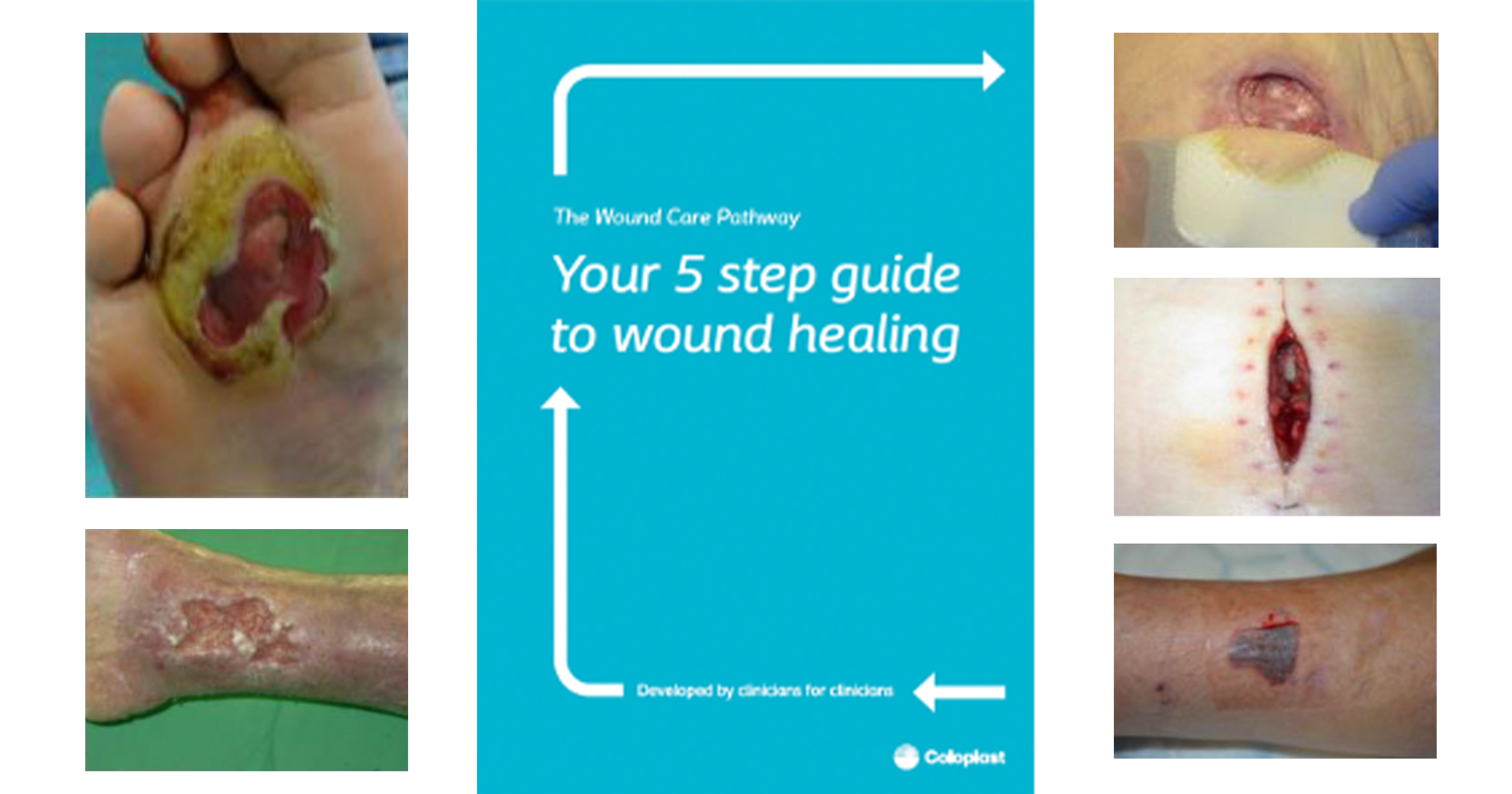
In 2020/21, an international consensus project was undertaken to create a systematic approach to healing chronic wounds. The result was the Wound Care Pathway developed by clinicians for clinicians (Dowsett et al, 2021; Figure 1). Incorporating feedback and input from over 2,200 healthcare professionals across more than 60 countries, the Wound Care Pathway offers a unique, step-by-step evidence-based approach to managing chronic wounds.
During conference symposiums and industry meetings, health care providers agreed that the Pathway will help lead to a shorter way to wound healing but asked for further guidance on specific wound types. A group of wound care experts, comprised of physicians, nurses and researchers, undertook a process to expand the international consensus on chronic wound care to focus on specific wound types. The objective was to utilise the mental model offered in the Wound Care Pathway to create a series of wound type specific pathways. Similar to the Wound Care Pathway, the wound type specific pathways took the latest complex research evidence and translated it into simple and practical treatment guidance for the non-specialist focused on wound healing, for the five most common wound types.
The most prevalent forms of wounds are diabetic foot ulcers, venous leg ulcers, pressure injuries/pressure ulcers, surgical wound dehiscence and skin tears (Frykberg and Banks, 2015; Guest et al, 2018; LeBlanc et al, 2018; Guest et al, 2020).
Diabetic foot ulcers (DFUs) are complex, chronic wounds (an example is shown in Figure 2), that have a major long-term impact on morbidity, mortality and quality of life. People with diabetes have a lifetime risk of foot ulceration of 19 to 34% with a yearly incidence rate of 2% (Bus et al, 2023). According to the International Diabetes Federation, persons with diabetes are up to 40 times more likely to require lower-extremity amputation compared to the general population. Approximately 85% of amputations are preceded by the development of a neuropathic foot ulcer (Wounds Canada, 2021). Unlike other chronic wounds, the development and progression of DFUs are often complicated by a wide range of changes related to the effects of diabetes mellitus, such as neuropathy and vascular disease (Wounds International, 2013).
The Scottish Intercollegiate Guidelines Network (SIGN, 2010) guide on the management of chronic venous leg ulcers (VLUs) describes VLUs as arising from venous valve incompetence and calf pump insufficiency, which leads to venous stasis and hypertension resulting in microcirculatory changes and localised tissue ischaemia. Chronic venous insufficiency leads to approximately 80% of lower leg ulcers (Evans et al, 2019). VLUs are common [Figure 3], often recurrent, painful and negatively affect quality of life. Unfortunately, VLUs have a long healing trajectory, with approximately 30% unhealed at 24 weeks (Evans et al, 2019).
The National Pressure Injury Advisory Panel (NPAIP, 2019) and the UK National Health Service (NHS, 2018) define pressure injuries/pressure ulcers (PI/PUs) [Figure 4] as localised damage to the skin and underlying soft tissue usually over a bony prominence or related to a medical or other device. The injury can present as intact skin or an open ulcer. The injury usually occurs as a result of sustained pressure, or pressure in combination with shear. The tolerance of soft tissue for pressure and shear may be affected by issues such as moisture, nutrition, comorbidities and condition of the skin. PI/PUs are painful for patients, costly for healthcare systems, are often very hard to heal and are largely preventable (Norton et al, 2017).
Surgical wound complications are one of the leading global causes of morbidity following surgery and continue to challenge health care professionals (Sandy-Hodgetts et al, 2020). In the UK, surgical wounds healing by secondary intention are common and account for 26–28% of all surgical wounds that require continued nursing intervention (Guest et al, 2018). Data from large community-based organisations in Canada representing wound patients (n=24,678) have demonstrated that 43.9% of the wounds being managed are surgical wounds healing by secondary intention. Patients with these wounds required nursing care and clinical support for 6–69 weeks (World Union of Wound Healing Societies; WUWHS, 2018). Surgical wound Dehiscence (SWD) [Figure 5] is defined as the rupture or splitting open of a previously closed surgical incision site and may be either superficial or deep, requiring healing by secondary intention (Mangram et al, 1999). SWD can occur at multiple regions, or involve the full length of the incision, may affect some or all tissue layers and may expose organs or implants (WUWHS, 2018).
The International Skin Tear Advisory Panel (ISTAP, 2018) defines a skin tear as a wound caused by shear, friction, and/or blunt force resulting in separation of skin layers. Skin Tears [Figure 6] often occur on patients with dermatoporosis, such as pathological skin aging (Bocheva et al, 2019). A skin tear can be partial-thickness (separation of the epidermis from the dermis) or full-thickness (separation of both the epidermis and dermis from underlying structures). Skin tears can be found on all areas of the body but are most often situated on the extremities. Skin tears are traditionally categorised as acute wounds, yet many reports indicate that skin tears fail to meet the expected wound healing milestones, resulting in the transition to chronic wounds, especially in older people, the very young and critically or chronically ill patients (LeBlanc et al, 2017).
The five Wound Type Specific Pathways provide step-by-step guidance tailored for the non-specialist on how to manage DFUs, VLUs, PI/PUs, SWDs and skin tears that is evidence-based and practical and when followed, will help lead to a shorter way to wound healing.
Methodology
This project was built on the ratified consensus created through the Wound Care Pathway development process and the resulting step-by-step critical thinking pathway that improved the way we think about wound care, wound healing and the patients’ involvement (Dowsett, 2019). The intent was to expand on the Wound Care Pathway by offering supplemental information specific to the five most common wound types — DFUs, VLUs, PI/PUs, SWDs and skin tears.
A panel of seven wound care experts from around the world governed the project and combined the experiential knowledge of health care professionals (HCPs), both specialist and non-specialists, with the latest research evidence. Five separate literature reviews were conducted [Tables 1 and 2]. The research evidence was reviewed by the expert panel and knowledge gaps were identified for further investigation. A global survey was designed to gather experiential evidence from healthcare providers to augment the research data. The survey was anonymous and was completed by 2,200 respondents, from 31 countries, across six continents and in eight languages [Figure 7]. Respondents included physicians (3%), nurse specialists (35%), general practice nurses (37%), and other HCPs, such as dietitians, chiropodists, physical and occupational therapists (25%).
Respondents reported that the five wound types chosen were in fact the most often seen wound types in their practice. This was especially the case for non-specialist respondents (clinic, home care and long-term care nurses and other HCPs). The majority of respondents (67%) reported that they usually or always work as part of an integrated/multidisciplinary team. When asked what percentage of chronic wounds they are currently treating that are healing, non-healing or non-healable, respondents indicated that the majority of their patients had chronic wounds that were healing (52%). Approximately a quarter of respondents indicated that the majority of their patient’s chronic wounds were non-healing (26%) and only 7% of respondents indicated that the majority of their patients’ wounds were non-healable.
The final stage of the process was a presentation of the five Wound Type Specific Pathways to specialist and non-specialist HCPs in six countries (Italy, France, UK, Germany, USA, Brazil), to seek feedback and reach consensus. A total of 62 HCPs participated in the focus group sessions — 55 nurses, five physicians and six other HCPs (i.e. physical therapists). Of the focus group participants, 89% agreed that providing wound type-specific guidance as a supplement to the Wound Care Pathway will help HCPs treat the most common wound types with evidence-based practices. The majority of participants agreed that the pathways were built on a strong evidence base and 84% indicated that using the pathways will lead to a shorter way to wound healing and have the potential to decrease the burden of wound care on health systems, HCPs and patients around the world [Figures 8 and 9].
The strength of the process was in the robustness of the research and experiential evidence gathering, the inclusivity of experts, specialists and non-specialists, and the global nature of the consensus reached. This depth and breadth of experience and input ensured that perspectives of the whole care team were considered and that those closest to the issue were included in the development of the guidance, a best practice common in the health quality improvement field (Jones et al, 2021).
Wound Type Specific Pathways
The purpose of the Wound Type Specific Pathways is to offer evidence-based guidance and solutions to non-specialist HCPs to help overcome the challenges often seen in DFUs, VLUs, PI/PUs, SWDs and Skin Tears. The Pathways can also be used by specialists to educate the non-specialist in evidence-based wound care practices. Each Pathway follows the Wound Care Pathway model to help HCPs assess, identify, understand, communicate and prevent/minimize risk factors that impede healing. Involvement of the patient as an active member of the integrated care team is emphasised throughout the Pathways and preventing complications and promoting wound healing are the focus for each wound type. Detailed guidance is also provided on when to refer patients.
Building on the Wound Care Pathway, the wound type specific pathways were developed to achieve the following objectives:
- Improve standards of care leading to a shorter way to wound healing
- Decrease inconsistencies of care, wound care costs and the time HCPs spend dealing with the most common types of chronic wounds.
- Provide evidence-based practice guidance to improve patient outcomes and quality of life for patients with DFUs, VLUs, PI/PUs, SWDs and skin tears
- Provide guidance to help HCPs focus on prevention of complications, further injuries and recurrence
- Provide clear, concise guidance to help non-specialist HCPs build confidence and implement best practice wound care at the bedside in a patient-centric manner.
Each Pathway defines the aetiology and features of the specific wound type, and then through a step-by-step approach provides guidance on:
- How to assess and diagnose the wound
- How to develop a treatment plan
- How to manage the wound
- How to choose a dressing and additional therapies
- How to monitor patients, wound progression and reduce complication and recurrence, and
- When to refer to a specialist.
Each pathway also offers reminders, tips and best practices for managing the specific wound types. Additional information and references are made available to the reader via QR Codes for deeper learning and for links to video demonstrations on techniques and procedures. Finally, each pathway includes clinical pictures and visual content to help guide the non-specialist through the process of identifying, assessing, treating and monitoring chronic wounds. All of this is provided in a visually simple step-by-step approach to assist generalist practitioners to manage chronic wounds of specific aetiologies effectively and efficiently, in collaboration with the patient and their integrated care team.
Table 2 provides highlights from the five wound type specific pathways, which will be available in electronic format November 2023, and in paper format and in multiple languages in 2024.
Conclusion
The Wound Type Specific Pathways, in conjunction with the original Wound Care Pathway, provides non-specialist HCPs with a practical evidence-based step-by-step approach to wound healing. Through easy-to-understand text, images and links to evidence details and educational videos, the pathways guide providers from identification, to assessment, diagnosis, treatment and monitoring, as well as offering tips on how to prevent and mitigate risks and when to refer. The pathways provide a holistic approach to healing wounds while preventing complications and further occurrence, by understanding the wound is on the patient and the patient is in their environment.
The five pathways were developed through a robust process of empirical and experiential evidence gathering and consensus-building deliberation that included researchers, thought-leaders, specialists and generalist practitioners. Building on the global consensus on chronic wound management that emphasised the importance of exudate and gap management, these wound type specific pathways guide HCPs when dealing with the risks and complications associated with DFUs, VLUs, PI/PUs, SWDs and Skin Tears. Implementing these Pathways can help improve the quality of wound care and patient outcomes, by focusing on wound healing. A focus on wound healing will help alleviate the global challenge of wound care for patients, society, healthcare systems and HCPs.