The term ‘leg ulcer’ is generally used to describe a full-thickness open wound below the knee with a slow healing tendency (Star, 2018). The two most common causes of leg ulceration (excluding the foot) are venous disease (venous leg ulcer, VLU) and arterial disease (arterial leg ulcer, ALU); other causes include diabetes, rheumatoid arthritis, vasculitis, sickle cell disease, malignancy and some pharmacological agents (e.g. corticosteroids) (National Institute for Health and Care Excellence (NICE), 2021). Many leg ulcers are caused by trauma (e.g. skin tears and avulsive injury) and are then exacerbated by the underlying disease state. Leg ulcers associated with more than one cause are commonly referred to as mixed aetiology leg ulcers. This paper focuses on the VLU.
Venous leg ulcers
A vast majority (70%) of lower-extremity ulcers are caused by chronic venous insufficiency (CVI). In the US and Europe, people >65 years of age are vulnerable to VLUs. The prevalence of VLUs is 1% of the population globally among those aged 18–64. In the US, 10–35% of the population suffer from chronic venous issues with 4% (>65 age group) of the cases having active ulcers (Sen, 2019). In the US, chronic venous disease alone causes at least 4.6 million lost work days and over $1 billion is being spent per year (Spentzouris and Labropoulos, 2009).
VLUs generally originate from minor traumatic injuries that do not follow the normal healing process as a consequence of CVI and the inflammatory status of the skin in the affected lower limbs (Meissner et al, 2007; Amato et al, 2015; Crawford et al, 2017; Mansilha and Sousa, 2018). They are typically associated with protracted healing, relatively high levels of exudation, malodour, pain, restricted mobility and sleep disturbance [Table 1]. Exacerbated by the high rate (50–70%) of recurrence of VLUs (Raffetto et al, 2021), these sequelae can have a negative impact on all aspects of daily living, causing depression, anxiety, social isolation and a decreased health-related quality of life (QoL) (Maddox, 2012; Green et al, 2014; Harding et al, 2015).
The direct costs associated with the management of patients with VLUs from the perspective of the UK’s National Health Service (NHS) have been estimated to be £7,706 per patient per year, which translates to an annual cost exceeding £2 billion when extrapolated to the UK population (Phillips et al, 2020). In the US, it has been estimated that the annual Medicare and commercial insurance costs associated with VLU treatment are close to $1 billion, with an annual US taxpayer burden of around $14.9 billion (Bradford Rice et al, 2014).
From a patient perspective, the results of numerous studies confirm a strong link between VLUs and reduced QoL. In one study, an analysis of data from nine patient interviews identified four core themes with 16 sub-themes that negatively impacted quality of life in physical, social and psychological domains [Figure 1]. Commenting on their findings, the researchers suggest that proactive symptom management and the fostering of a patient focus in consultations may improve QoL and encourage the patient to engage as an active partner in the management plan. More recently, a systematic review of relevant national and international articles published from 2012 to 2016 confirmed that VLUs “act on patients’ bio-psycho-social-spiritual and socioeconomic spheres, having a negative impact on their quality of life” (Joaquim et al, 2018).
Management of VLUs from a quality-of-life perspective
It is important that clinicians follow a systematic and holistic approach when assessing and managing patients with VLUs. The use of an assessment tool, such as the mnemonic HEIDI (History, Examination, Investigation, Diagnosis and Indicators) can help to identify the most appropriate supporting treatments (e.g. compression) and local treatments for ulcers (Harding et al, 2007). Applying the principles of the concept known by the mnemonic MOIST (Moisture balance, Oxygen balance, Infection control, Supporting strategies, Tissue management) can help to optimise the local treatment of chronic wounds, such as VLUs (Dissemond et al, 2014) [Figure 2].
The main goals of VLU treatment are to reverse the underlying venous hypertension and the pro-inflammatory environment (Chi and Raffetto, 2015).
Addressing CVI and venous hypertension
Compression therapy remains the gold standard of the conservative treatment of CVI in all stages, because of its non-invasive nature, ease of use, and efficacy in reducing venous hypertension, which is a main pathophysiological mechanism of CVI (Tkaczyk et al, 2021). In the presence of venous hypertension, the increase in lymphatic flow can overwhelm the lymph transport capacity, leading to phlebolymphoedema, Compression therapy is one of the most commonly employed interventions to manage patients with phlebolymphoedema (Ratcliff et al, 2022).
A number of different devices are used to apply compression; these include short-stretch bandages, long-stretch bandages, multi-layered bandages, hosiery (stockings), juxtaposed strap devices and pumps. Appropriate and correctly applied compression can help to reduce the diameter of veins, return blood to the central circulation and reduce oedema (Fletcher et al, 2013). Published in 2021, the results of a systematic review highlighted that people wearing compression bandages or stockings will probably experience a shorter time to complete healing of VLUs, are more likely to experience completed ulcer healing within 12 months, have less pain and better disease-specific QoL compared to those not using compression (Shi et al, 2021).
Although dressings do not play a direct role in this aspect of VLU management, it is important that clinicians select dressings that (i) have been designed and tested to confirm that their performance is not adversely affected by the mechanical forces imparted by the compression systems and (ii) do not interfere with the delivery of compression to the lower limbs. While compression is utilised in the majority of VLU patients, the reality is that adequate compression may not be achievable for all patients. For some patients, there is an absolute contraindication, such as the presence of severe peripheral arterial disease. There is also a large percentage of patients in whom inadequate compression is related to the inability to don and doff stockings or devices due to body habitus, manual dexterity or lack of strength. It is important to view these patients as challenges, rather than non-compliant, and attempt to find an effective level of compression. In the absolute absence of the ability to use applied compression, the use of pumps or looser tubular bandaging coupled with frequent leg elevation may be the required compromise. This places even greater importance on the selection of appropriate dressings to help manage the sequelae of VLUs described below.
Managing excess exudate (avoiding leakage) and malodour
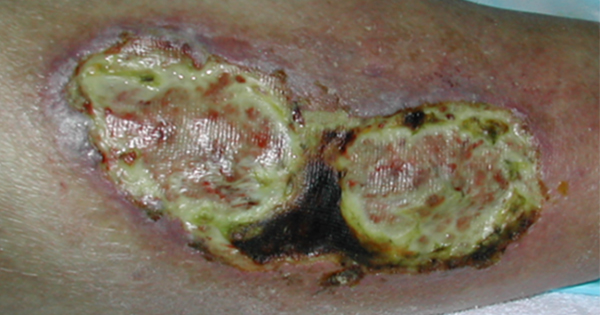
Inflammation following injury increases the permeability of capillaries which allows exudate to leak into the tissue and the wound bed. Composed of water, nutrients, inflammatory mediators, electrolytes, white cells, enzymes (e.g. proteinases) and growth factors, wound exudate plays an important role in the normal healing process. Generally, as a wound heals, exudate levels reduce. However, exudate may become a problem when the quantity produced increases, its consistency changes (e.g. increased viscosity) and/or its composition changes (e.g. increased levels of harmful metalloproteinases (MMPs)), which can delay healing, cause physical and psychosocial morbidity, and increase demand on healthcare resources. In common with many other chronic wound types, VLUs often present with excessive exudation which, if not managed optimally, may damage the wound bed and periwound skin (e.g. maceration and excoriation). Excessive exudate which has drained onto an outer dressing or clothing may begin to develop an odour if allowed to persist. Malodour that remains after a dressing is removed and the wound and periwound skin is cleansed may be indicative of increasing bioburden or potential infection (WUWHS, 2019).
Dressings play an important role in the management of excess exudate. In doing so, they should be (i) able to handle exudate and its components through absorption, moisture vapour loss and retention, even when working against gravitational forces and the mechanical forces applied by compression systems, (ii) capable of reducing the risk of leakage and spread of exudate onto the periwound region (reducing the risk of maceration and skin erosion) and, (iii) act as a barrier against the invasion of microorganism. Dressings should also be designed to stay securely in place — size, shape, propensity to adhere to the wound and surrounding skin, and ability to conform to different anatomical locations are some of the properties that determine the durability (‘wear time’) of dressings. The term ‘strikethrough’ is commonly used to describe the point in time at which a dressing no longer stays sealed over the wound or exudate has penetrated through the surface of the dressing, causing leakage [Figure 3]. Strikethrough can be caused by saturation, loss of edge seal/adherence, dislodgement due to friction or movement, and/or a defect in the dressing (Alvarez et al, 2021).
Leakage and malodour cause considerable distress to patients and their carers. This was explored in a mixed method study, in which both quantitative (Hospital Anxiety Depression Scale and qualitative (interviews) data were analysed to investigate the link between depression and VLU-associated exudate and malodour. Respondents reported adverse effects of excessive exudate and malodour on their psychological wellbeing, leading to feelings of disgust, self-loathing and low self-esteem (Jones et al, 2006; 2008). Commenting on these findings, the researchers describe how the stigma associated with leakage and malodour can lead to patients withdrawing from activities (such as work or going out socially) to avoid embarrassment (Jones et al, 2008). In a later study which was undertaken to understand the personal impact of VLUs from the perspective of patients, the impact of exudate (e.g. leakage) and malodour was described as devastating, causing embarrassment, shame and stress. Some patients reported that they tried to manage this situation by limiting their contact with others and creating a self-imposed isolation (Green et al, 2013).
In an earlier study, participants viewed exudate and malodour as ‘unbearable’ and expressed concerns about exudate coming into contact with their clothes and household furnishings (Rich and McLachlan, 2003). Leaking and soiling can be extremely distressing to patients and their carers. The increased need for washing of clothing and bedlinen is a burden that patients and carers can do without (WUWHS, 2019). In a survey involving over 2,000 patients from 15 countries, 64% of respondents revealed that leakage was a problem for them (Price et al, 2008). Box 1 lists some published feedback obtained from patients that clearly highlight the devastating impact of leakage. Leakage may also increase the risk of infection by providing a portal of entry into the wound environment which is conducive to microbial colonisation and a nidus for potential infection (WUWHS, 2019) and lead to moisture-related damage (e.g. maceration, erosion) of the skin around the ulcer. This can cause delays to the healing of ulcers and have a negative impact on the well-being of patients.
Managing wound pain
Wound-related pain is multidimensional; it integrates the experience of chronic wound pain (i.e. the persistent pain that is usually associated with the underlying wound aetiology) with cyclic acute pain (i.e. the periodic pain that is induced by repeated interventions such as recurring dressing changes) and non-cyclic acute pain (i.e. single-episode pain arising from procedures such as sharp debridement (Krasner, 1995). Historically, dressing removal was regarded as the most painful wound care intervention for patients, primarily due to direct adherence of dressings to wounds and dressings drying out (Kammerlander and Eberlein, 2002). For example, in a survey involving over 2,000 patients from 15 countries, over 40% of respondents revealed that pain at dressing change was the worst part of living with a wound (Price et al, 2008).
Acute pain experienced at dressing changes has the potential to cause psychological stress [Figure 4], which, in turn can trigger a number of unwanted consequences such as adverse effects on physical health and many physiological processes, delayed healing and reduced QoL (Upton et al, 2012). These observations highlight the importance of selecting dressings that are known to be atraumatic on removal, such as those with soft silicone wound-skin contact surfaces that adhere to intact dry skin and will remain in situ on the surface of a moist wound or damaged periwound skin without adhering to the fragile tissues, thus minimising pain at dressing changes (Woo et al, 2009).
Managing infection
VLUs are susceptible to microbial invasion and infection. The presence of infection can lead to increases in exudation, malodour and pain, therefore, adding unwanted complexity to the management of these sequelae. Ulcer enlargement and delayed healing will likely follow. Because the presence of VLUs can have a profound effect on the wellbeing of patients, the longer a VLU is present, the greater its impact on the patient will be (Parker et al, 2015). Prevention of infection in VLUs is, therefore, of paramount importance. If infection does occur, then it should be treated according to clinical guidelines (e.g. topical antimicrobials versus systemic antibiotics). Clinicians can consider the adjunctive use of dressings incorporating antimicrobial agents (e.g. sliver) if indicated.
Avoiding unnecessary dressing changes
Dressing wear time is related to the type of dressing used, the condition of the wound and its surroundings, and clinical protocol-specified change frequency. In some respects, a dressing change can be viewed as a ‘disturbance’ to the wound. While there are circumstances when it is absolutely necessary to ‘disturb’ wounds for inspection (e.g. to monitor for signs of infection) or management (e.g. debridement) or when a dressing is nearing or has reached strikethrough (i.e. leaking), too many disturbances to wounds can delay healing or even lead to adverse events, such as introducing infection, damaging the periwound skin and increasing the risk of adhesive dressing-related skin injuries (Davies et al, 2019). As dressing design continues to develop (i.e. enhanced fluid handling capacities, improved adhesion), clinicians have the option of leaving some dressing types in place for longer periods than possibly historically, thereby adopting the concept of ‘undisturbed wound healing’ and avoiding unnecessary high-frequency dressing changes.
From a VLU perspective, the ‘ideal’ dressing would need to provide effective exudate management and stay securely in place for the entire period during which bandages/stockings are in place, thereby preventing any interruption in the delivery of compression. As research has identified that signs of psychological stress increase during dressing change procedures for patients with chronic wounds (Upton et al, 2012), appropriate implementation of the undisturbed wound healing concept should be considered as a means of improving the wellbeing of patients with VLUs.
Of primary importance is keeping the patient as the key focus in the care. Creating an environment of trust and open communication is essential to the impact that the disease, the ulcer, and the management decisions may have. Asking open ended questions related to their pain, for example, not just a number, but how it affects their life, their appetite and sleep. Further querying about the comfort of the compression or the dressing, or any potential change in the treatment plan that can improve their day to day life as they continue on the journey will confirm that the clinician is invested in not only their healing but in their overall wellbeing.
Conclusions
As well as being challenging clinically and economically, VLUs cause patients a wide range of psychosocial issues including depression, anxiety and social isolation. While the underlying causes of VLUs can be effectively addressed with the use of compression therapy, it is equally or more important for clinicians to provide appropriate local ulcer management to minimise the impact that high exudation (e.g. leakage and maceration), malodour, pain and frequent dressing changes can have on the health-related QoL of patients (e.g. embarrassment, distress and self-isolation). The selection of dressings that can perform in conjunction with compression therapy, manage the high levels of exudate, minimising the risk of leakage and malodour typically associated with VLUs, minimise dressing-related pain and trauma, and avoid the need for unnecessarily frequent dressing changes is key to delivering the quality of care that patients deserve.