1. Foreword
Pressure injuries, also referred to as pressure ulcers, pressure sores, bedsores or decubitus ulcers (Wound, Ostomy and Continence Nurses Society; WOCN, 2017), are a common and preventable health problem. They impose significant health and economic burdens on patients, caregivers and healthcare systems. For the patient, pressure injuries can have a major impact on quality of life and mortality, with personal burdens ranging from pain and discomfort to psychosocial sequelae including stress, anxiety and depression, as well as declines in autonomy, security, spiritual wellbeing and social functioning (Gorecki et al, 2012; WOCN, 2017; European Pressure Ulcer Advisory Panel (EPUAP), National Pressure Injury Advisory Panel (NPIAP) and Pan Pacific Pressure Injury Alliance (PPPIA), 2019a).
Evidence-based pressure injury management can prevent infection, facilitate optimal wound healing, minimise scarring and prevent serious consequences such as morbidity and mortality. Achieving success in pressure injury management requires skill and knowledge. However, a significant challenge faced by clinicians is wound management, which is complicated by the diverse clinical effects and cost efficiency of various treatment methods and preventive approaches for these types of wounds.
In recognition of clinicians’ need for guidance on pressure injury management in Australia, an advisory group of national experts was formed in June 2021. The aim of the group was to develop a simplified clinical decision guide for the assessment and management of pressure injuries that should be used in daily practice alongside existing international guidelines. The advisory group comprised 12 members all with broad and specialised experience in clinical practice and research pertaining to pressure injury prevention and management. The group was named PITA (Australian Pressure Injury Treatment Advisory) group and convened four times, during which a consensus was achieved on the contents of a ‘Quick Guide’ to Pressure Injury Management.
Recognising the importance of aligning with established guidelines, the PITA group ensured that their scope extended beyond treatment alone and therefore actively incorporated assessment and prevention into their agenda and discussions. The PITA ‘Quick Guide’ to Pressure Injury Management follows current clinical evidence, best practice guidelines and implementation documents regarding the treatment of pressure injuries. It supports the current international guideline by providing a practical ‘how to’ guide for clinicians. The intent of this new guide is to provide a simplified and up-to-date resource that is quick and easy-to-use in the assessment and management of pressure injuries. This ‘Quick Guide’ is targeted at all clinicians responsible for the management of pressure injuries.
It is important to note that the recommendations in this ‘Quick Guide’ may not be suitable for use in all circumstances. The Australian PITA group developed this ‘Quick Guide’ based on evidence-based clinical recommendations, but any healthcare professional using it should also refer to the most recent international guidelines and conduct a holistic assessment of the person with a wound.
2. Introduction
Pathogenesis of pressure injuries
A pressure injury is defined as an area of localised injury or damage to the skin and/or underlying soft tissue that typically occurs over a bony prominence, resulting from pressure or pressure in combination with shear and/or friction (EPUAP/NPIAP/PPPIA, 2019a). Pressure injuries lead to tissue and cell deformation as well as ischemia, lymphatic flow blockage and reperfusion damage (Santamaria et al, 2018; EPUAP/NPIAP/PPPIA, 2019a; Wilson et al, 2019; Gefen et al, 2022). The severity of these injuries is proportional to the magnitude and duration of deformation, and in some cases, they can occur very rapidly (Gefen et al, 2022).
A pressure injury may also be related to the use of a device, in which case it is referred to as a device-related pressure injury (DRPI; Gefen et al, 2022).
Terminology
As highlighted by the 2019 international guideline on pressure injury/ulcer prevention and treatment (EPUAP/NPIAP/PPPIA, 2019a), there is ongoing discussion around pressure injury terminology. The original term, ‘gangraena per decubitum’ meaning ‘dead tissue due to lying down’ was coined by Wohlleben in 1777. The associated term ‘decubitus’ was first used to describe wounds related to bed rest. Later in the 19th century, the term ‘bedsore’ was commonly used, followed by ‘pressure sore’ and ‘pressure ulcer’ in the 1980s and 1990s, respectively. While these terms are still commonly used, they do not accurately reflect the aetiology of the injury. The words ‘sore’ and ‘ulcer’ imply an open wound at the skin surface (EPUAP/NPIAP/PPPIA, 2019a), whereas the NPIAP pressure injury system, the most widely accepted pressure injury classification system, defines a Stage I pressure injury as ‘non-blanchable erythema of intact skin’ (Edsberg et al, 2016).
The term ‘pressure ulcer’ is still widely used in Europe, while ‘pressure injury’ is now widely adopted in South-East Asia, Australia and New Zealand, with the United States of America following suit (EPUAP/NPIAP/PPPIA, 2019a). In this ‘Quick Guide’, the term ‘pressure injury’ will be used throughout.
Pressure injury stages
Staging systems are used to classify and describe pressure injuries according to the extent of tissue loss and physical appearance of the injury (Edsberg et al, 2016). While all pressure injuries are serious, their severity can vary in terms of clinical impact and treatment difficulty, ranging from patches of discoloured skin that may heal to deep open ulcers that expose the underlying bone or muscle, which may be very challenging to treat (EPUAP/NPIAP/PPPIA, 2019a).
Pressure injury classification is based on the visual and palpatory identification of various tissue layers, including skin, subcutaneous fat, bone, muscle, tendon and ligament (EPUAP/NPIAP/PPPIA, 2019a). Pressure injuries are categorised into four stages (Stages 1–4), with higher stages indicating more tissue damage and associated economic costs. There are also two additional stages, namely unstageable pressure injury (covered in eschar or slough) and suspected deep tissue injury (Edsberg et al, 2016).
Dark skin tones
It is acknowledged that identifying early changes in skin colour which may indicate a Stage 1 pressure injury or deep tissue injury can be difficult in individuals with dark skin tones (Black and Simende, 2020). These groups are at a higher risk of developing pressure injuries and have been reported to have higher rates of full-thickness pressure injuries and increased mortality associated with these wounds (Bauer et al, 2016). Additionally, there is a frequent use of light skin tone examples in teaching and learning about pressure injuries in undergraduate and postgraduate nurse education (Gunowa et al, 2021). Due to these factors, the PITA group recommends giving additional consideration in the assessment of skin in individuals with dark skin tones.
Impact on the individual
Complications of pressure injuries can be serious and have a negative impact on individuals, their families and healthcare services. These impacts include loss of mobility, independence, privacy, dignity and ability to engage in preferred activities (Jackson et al, 2018), as well as severe pain, increased risk of infection (Edsberg et al, 2016) and delayed wound healing.
Prevention
Pressure injury prevention is the most important step in the prevention and management of these difficult-to-treat wounds, with the initial stage involving an assessment of the individual’s risk status (Boyko et al, 2018; Al Aboud and Manna, 2022). Prevention of pressure injuries involves alleviating risk factors for the individual and minimising episodes of prolonged pressure. This can be achieved by placing pressure redistributing or off-loading devices/dressings at pressure points or by frequently repositioning the patient (Boyko et al, 2018). When developing an individual care plan, it is crucial to consider additional preventative measures, including implementing skincare and hygiene regimens, continence management, using appropriate bed linen to minimise the shear effect, prophylactic dressings, mobilisation support surfaces, as well as optimising nutrition and hydration (EPUAP/NPIAP/PPPIA, 2019a). These preventative measures should be carefully considered and implemented based on each patient’s assessment outcomes.
Treatment
When a pressure injury occurs, treatment is critical to promote healing and minimise the risk of complications (Qaseem et al, 2015). While the impact of a pressure injury might exhibit similarities across individuals, the primary concerns will vary from person to person. Hence, addressing these concerns will require involvement of the multidisciplinary team for a holistic care approach (Jackson et al, 2018). As defined by Qaseem et al (2015), a multidisciplinary approach involves nurses, physicians, dietitians, allied health and other members of a care team. Further, this care may be provided in a wide range of settings, including in the community, hospital or residential care and by a variety of healthcare providers (Qaseem et al, 2015; EPUAP/NPIAP/PPPIA, 2019a).
The goal of all treatment options is to minimise the pressure exerted on the wound and reduce moisture while maintaining an aseptic or least septic environment as possible (Zaidi and Sharma, 2022). The choice of treatment options should be according to the stage of the injury and the intended purpose of treatment, such as reducing moisture, removing necrotic tissue and/or controlling bacteraemia (Zaidi and Sharma, 2022). Treatment interventions may include managing underlying risk factors, using support surfaces, providing nutritional support, implementing specific wound care regimens and adjunctive therapies, and, if necessary, performing surgical repair (National Institute for Health and Care Excellence, 2014; Qaseem et al, 2015).
Superficial pressure injuries are typically expected to show signs of healing within two weeks, however, there are cases where this may not occur and the wound may deteriorate (NPIAP/EPUAP/PPPIA, 2014; Westby et al, 2017; EPUAP/NPIAP/PPPIA, 2019a). According to the 2019 international guideline (EPUAP/NPIAP/PPPIA, 2019a), if a pressure injury does not show any signs of healing within two weeks despite appropriate local wound care, pressure distribution and nutrition, a comprehensive reassessment of the individual should be conducted.
There are many treatment options available, including wound dressings and topical agents such as ointments, creams and gels (Westby et al, 2017). However, evidence supporting the effectiveness of specific dressings and topical agents in aiding the healing of pressure injuries is limited (Westby et al, 2017). According to the 2019 international guideline (EPUAP/NPIAP/PPPIA, 2019a), adjunctive therapies may be considered in cases where wounds are not progressing adequately or where chronic osteomyelitis is present (Boyko et al, 2018). Examples of adjunctive therapies include electrotherapy, ultrasound therapy, negative pressure wound therapy (NPWT), oxygen therapy or surgical repair of the wound.
Moreover, many novice clinicians find pressure injury prevention, assessment and treatment interventions confusing and overwhelming due to the plethora of products available (Barakat-Johnson et al, 2019a; Li et al, 2022). Approaches to pressure injury treatment are dependent on the expertise of the individual, with novice clinicians relying on experts to review the wound and provide guidance on wound management (Welsh, 2018). Additionally, access and equity to these products across all clinical settings is highly variable and further complicates decision-making.
Wounds that are not progressing adequately require clinicians to have a thorough understanding of evidence-based interventions and access to resources to avoid further deterioration. The PITA group acknowledges the importance of assessment and prevention as part of pressure injury management; however, there is a lack of clear and useful guidance focusing on pressure injury treatment. Clinicians may also find existing guidelines difficult to use, or with a lack of clear visual aids (Qaseem et al, 2015; Tachibana et al, 2016; WOCN, 2017; Atkin et al, 2019; EPUAP/NPIAP/PPPIA, 2019a; EPUAP/NPIAP/PPPIA, 2019b; Gefen et al, 2020; Kirman, 2020).
3. Prevention and Treatment of Pressure Injuries: 2019 International Clinical Practice Guideline
In 2019, the EPUAP, NPIAP and PPPIA published the third edition of the Prevention and Treatment of Pressure Ulcers/Injuries: Clinical Practice Guideline. The international guideline presents a comprehensive review and evaluation of the best available evidence (at the time of the literature search), followed by 114 recommendations and 62 best practice statements to guide practitioners in risk assessment, diagnosis, prevention and treatment of pressure injuries.
Furthermore, the guideline considers the specific needs of different population groups and emphasises the importance of considering the patient’s perspective. It provides recommendations for supporting and involving patients in their care, as well as 20 quality indicators aimed at monitoring the implementation of the international guideline recommendations (EPUAP/NPIAP/PPPIA, 2019a).
One concise publication that summaries the content of the full international guideline (EPUAP/NPIAP/PPPIA, 2019a) is the Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide (EPUAP/NPIAP/PPPIA, 2019b).
4. Further considerations in developing the PITA ‘Quick Guide’
Risk factors for pressure injury
The risk factors associated with pressure injury development should be carefully considered. Identifying individuals who are at risk of developing pressure injuries through risk screening is a central component of clinical practice (EPUAP/NPIAP/PPPIA, 2019a). It is important to note that an individual’s risk of pressure injury may change with alterations in their health status and these changes can occur over time. Therefore, it is important to screen patients upon admission, assess their risk when identified and regularly monitor them, especially when there is a change in their health status (EPUAP/NPIAP/PPPIA, 2019a). Another significant component in pressure injury prevention, classification, diagnosis and treatment is the assessment of the skin and soft tissues (EPUAP/NPIAP/PPPIA, 2019a). Clinicians use visual inspection and tactile examination to assess the individual’s skin appearance, integrity and underlying tissue health. This assessment is not limited to the site of the injury alone; it extends to surrounding areas which might also exhibit early signs of damage.
For patients identified as being at risk of developing pressure injuries or those already experiencing pressure injuries, evidence-based guidelines should be used to ensure that appropriate preventative and treatment interventions are implemented (WOCN, 2017).
Device-related pressure injury
Devices can include a wide range of items, such as oxygen tubing, endotracheal tubes, bite blocks, orogastric and nasogastric tubes, urinary catheters and faecal containment devices. Device-related pressure injuries (DRPIs) can occur either on the skin or mucous membrane (Gefen et al, 2022). However, pressure injury classification systems are designed for injuries on the skin and are not applicable to the mucous membrane, as the mucosa is anatomically different. Instead, pressure injuries on the mucous membrane are not staged but documented as mucosal pressure injuries.
According to the 2019 international guideline (EPUAP/NPIAP/PPPIA, 2019a), all patients with a device should be considered at risk for DRPIs. It is recommended to inspect the surrounding skin and skin beneath any device at least twice a day, and more frequently if the patient is at high–risk. Additionally, any potential device-related sources of pressure should be removed as soon as medically possible (Galetto et al, 2021). The overall treatment goals for DRPIs occurring on the skin are similar to those for pressure injuries that result from pressure, shear and/or friction.
Critically ill individuals admitted to intensive care are particularly vulnerable to pressure injuries (Lovegrove et al, 2020) due to their limited mobility, compromised cognition and reduced sensation often caused by sedation and the presence of multiple medical devices.
A modified Delphi study (Lovegrove et al, 2020) was conducted to determine the essential preventative interventions for pressure injuries in critically ill patients based on their risk levels, yielding several recommendations. As per the study, all patients should undergo a risk screening within two hours of admission and receive regular risk screening every eight hours. Patients identified as moderate– to high–risk should be provided with an appropriate mattress support surface based on their risk screening, as well as a device to offload pressure from the heels. High–risk patients should also receive nutritional supplements if able to eat orally or parenteral nutritional support if unable to do so. Furthermore, the study suggests using five-layered silicone foam dressings for sacral, heel and trochanteric areas, an active mattress support surface and a pressure-distributing cushion for sitting. The Delphi panel also agreed that repositioning should be performed at least every four hours for low–risk patients and every two hours for moderate– and high–risk patients, irrespective of the mattress device or the use of slide sheets and other resources (Lovegrove et al, 2020).
The SECURE acronym for the prevention and treatment of DRPIs (Gefen et al, 2022) is an excellent tool to help guide a clinician’s assessment and prevention plan [Table 1].
Cost
While directly comparing health economic data across different geographic locations can be challenging, pressure injuries present a substantial financial burden on healthcare systems. They are associated with increased length of hospital stay, readmissions and high financial costs of care (Chaboyer et al, 2016; EPUAP/NPIAP/PPPIA, 2019a).
Pressure Injuries pose a significant cost to the health system (Graves and Zheng, 2014a, 2014b; Norman et al, 2016). In a recent study on costings in Australia, the cost of pressure injuries amounted to AUS$9.11 billion annually with extended hospital stays accounting for AUS$3.60 billion and treatments costing AUS$3.59 billion (Nghiem et al, 2022).
In the US, the cost of a hospital-acquired pressure injury (HAPI) is approximately US$10,708 per person, resulting in a total that exceeds approximately US$26.8 billion (Padula and Delarmente, 2019).
Person-centred care
Within the field of wound care, there is an increasing emphasis on engaging patients in their care. The terms ‘person-centred’ and ‘patient-centred’ are often used interchangeably and have gained significant attention in recent years, supported by emerging evidence in the field of wound management (Gethin et al, 2020). This approach aims to facilitate the implementation of care practices and strategies that are important for patient safety, which may be less effective without full patient engagement (McInnes et al, 2014). It is thought that when patients are actively engaged and involved in their care, the delivery of pressure injury prevention regimens can potentially reduce financial and physical burdens, ultimately improving patient outcomes (McInnes et al, 2014).
This shift towards person-centred care is driven, in part, by the growing public interest in understanding diseases, symptoms and treatment options. With the aid of social media, patient networks and new technologies, individuals are now seeking more information about their own health conditions or those of their family members (Gethin et al, 2020). As highlighted by Gethin et al (2020), this growing interest and engagement in person-centred care has allowed healthcare providers to tap into patients’ knowledge and expertise, which is arguably an underutilised resource in care settings. Numerous organisations have embraced this care approach and policy reforms and approaches have been implemented to support person-centred care and integrated health services (Whitty et al, 2017; Gethin et al, 2020).
Person-centred care includes patients as partners in their own care, with a focus on keeping the patient’s individual needs remaining at the centre of the decision-making process (Gethin et al, 2020). Importantly, according to the person-centred care concept, a patient should not be defined by their health condition; and their plans, beliefs, strengths and personality should be carefully considered (Gethin et al, 2020).
From a nursing perspective, person-centred care is a multi-dimensional concept and includes promoting patient participation and autonomy, shared decision-making, shared power, knowledge sharing, caring attitudes and individualising patient care (Lusk and Fater, 2013; Latimer et al, 2014; Gethin et al, 2020). Ultimately, person-centred care aims to establish respectful and collaborative partnerships between healthcare professionals and patients (Latimer et al, 2014).
There are several factors that may hinder patient involvement in patient safety and care. According to McInnes et al (2014), successful patient participation in pressure injury prevention requires ongoing education throughout their admission, effective pain and discomfort management and the establishment of a supportive and collaborative relationship with healthcare staff working in partnership with the patients. Engaging patients in their care can be a complex task, particularly for those with chronic wounds, as it often signifies a wider systemic disease that necessitates an interdisciplinary approach involving several healthcare professionals and services (Norman et al, 2016). This complexity can increase the risk of communication issues and possible treatment failures at various points along the patient’s care journey (Lindsay et al, 2017). Moreover, the treatment process for patients with chronic wounds may be made increasingly difficult due to limitations and inconsistencies in patient health literacy, leading to uncertainty about what to expect during their care journey (Lindsay et al, 2017).
Lindsay et al (2017) additionally highlight the core concept of person-centred care and how its application necessitates a holistic approach that considers the individual as a whole, beyond just their wound. Person-centred care is based on individualised care and involves a collaborative approach in which patients are encouraged to be equal partners and healthcare professionals can learn from the patient’s experiences (Lindsay et al, 2017). Central to this concept is effective communication, language and terminology, education and patient advocacy (Lindsay et al, 2017).
Latimer et al (2014) investigated patient preferences for involvement in pressure injury prevention, highlighting the complexities and barriers associated with patient involvement. Patient involvement cannot be assumed, as it can range from non-participation to active participation. It is important to recognise that not all patients are able or willing to actively participate in their care; as some patients may prefer or require a more passive role (Latimer et al, 2014). This further highlights the importance of individualising care on a patient-by-patient basis.
Crucially, in order to form effective partnerships, the patient’s role must first be clearly defined. Additionally, it is important to identify barriers and challenges to implementing these partnerships and develop strategies, including educational tools, to overcome them (Latimer et al, 2014). A willingness and understanding of how to actively participate, from both the perspectives of the patient and healthcare workers, effective leadership and a cultural shift to reorganise healthcare processes are all fundamental elements of person-centred care (Gethin et al, 2020).
Implementation of care bundles in pressure injury prevention and management
Multicomponent and person-centred care bundles are increasingly recognised as important strategies in pressure injury prevention, with research demonstrating their role and value in nursing care (Chaboyer et al, 2016; Whitty et al, 2017).
Several studies have also highlighted the need for careful consideration in implementing pressure injury prevention and management strategies. Barakat-Johnson et al (2019a) explored the thoughts and experiences of hospital nurses involved in pressure injury prevention and management. They found that difficulties exist when it comes to delivering quality care due to competing priorities and challenges faced at both the organisational and patient levels. The study concluded that pressure injury prevention and management should not be viewed in isolation, as it is only one aspect of patient care. Hospitals must implement measures to support and enable nurses to deliver quality care in pressure injury prevention and management (Barakat-Johnson, 2019a).
Processes used to implement evidence-based practice play a significant role in influencing outcomes (Barakat-Johnson, 2019b). In 2016, Sving et al highlighted the need to increase knowledge about adequate implementation strategies related to pressure injury prevention. As such, they conducted a study to evaluate whether a multi-faceted, unit-tailored intervention using evidence-based pressure injury prevention affects the prevention and prevalence of pressure injury and the nurses’ knowledge and attitudes. The study used the Promoting Action on Research Implementation in Health Service (PARIHS) framework to identify key implementation areas and guide the planning and evaluation of the intervention (Harvey and Kitson, 2016). They found that statistically significantly more patients received pressure ulcer prevention care following the intervention (Sving et al, 2016).
A significant increase in HAPIs over a five-year period in one Australian health district was the catalyst for the use of the PARIHS framework. Barakat-Johnson et al (2019b) demonstrated the importance of the framework in understanding the translation of evidence in a complex health system and how it helped in mapping elements that could potentially influence implementation outcomes.
Tayyib and Coyer (2016) reported on the successful implementation process used to integrate a pressure injury prevention care bundle approach for improving patients’ skin integrity in intensive care. The care bundle demonstrated a significant reduction in pressure injury incidence, using the Ottawa model of research use as a consolidated framework for implementing bundled evidence into daily clinical nursing practice (Tayyib and Coyer, 2016).
Barakat-Johnson et al (2019c) also highlighted how patient care planning should incorporate the timely implementation of evidence-based strategies in terms of lowering rates of HAPIs and associated skin conditions. In a study conducted in an Australian local health district, the costs of HAPIs were determined and compared with the costs and outcomes of a program implemented to reduce HAPI incidence. The study found that HAPI intervention-based program resulted in a reduction in HAPI incidence and prevalence within the local health district. Furthermore, the program and its implementation helped reduce costs associated with HAPIs compared to the previous approach to preventing HAPIs in one local health district (Barakat-Johnson et al, 2019c).
5. Pressure injury prevention, assessment and staging (clinical decision tree)
To aid clinicians in the prevention, staging, assessment and determination of care goals for individuals with pressure injuries, the PITA group developed a Clinical Decision Tree [Figure 1, page 11]. This tool will help clinicians create the most appropriate treatment plan and ensure that pressure injuries are appropriately evaluated, reported and documented, taking into account local guidelines and policies.
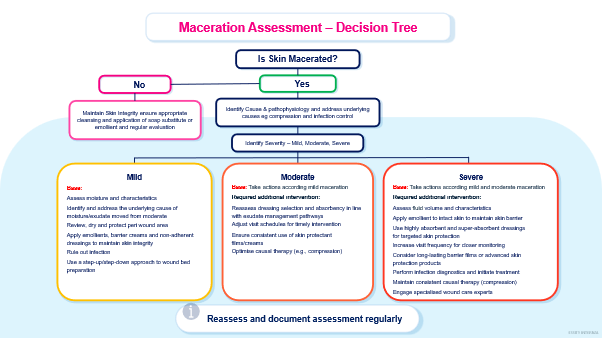
6. Quick guide to pressure injury management
The ‘Quick Guide to Pressure Injury Management’ tool [Figure 2, pages 12–14] aims to support clinicians in formulating the most suitable treatment plan. This guide, developed by the PITA group, takes into consideration treatment aims, patient-related factors, wound characteristics and recommended products.
Prevention and management of pressure injuries necessitate a multidisciplinary team approach due to the wide-ranging impact of these injuries. To ensure optimal treatment, the following factors should be taken into consideration [Table 2, page 15].
Disclaimer
The decision to adopt any recommendation must be made by the qualified healthcare professional, taking into consideration available resources and the individual patient’s circumstances.
The Australian PITA Group is unable to guarantee the reliability and accuracy of the individual studies referenced in this ‘Quick Guide’.
Nothing in this ‘Quick Guide’ should be considered as medical advice for specific cases.
This ‘Quick Guide’ is intended for educational and informational purposes only. The information contained within was deemed accurate by the Australian PITA Group at the time of publication.
It is important to note that research, technology and clinical guidance are subject to rapid change, and the recommendations in this ‘Quick Guide’ may become inconsistent with future advances.
The healthcare professional is responsible for staying informed about research and technological advancements that may impact their clinical decision-making.
This ‘Quick Guide’ is not intended to endorse any specific product or solution; as such, generic names of products and solutions have been used throughout this ‘Quick Guide’.
This ‘Quick Guide’ does not provide advice on reimbursement regulations.
This ‘Quick Guide’ is not intended to provide full safety and usage information for products, devices or solutions. Any product, device or solution mentioned should be used in accordance with the relevant manufacturer’s instructions for use and any caution statements related to those products, devices or solutions should be observed (including any data related to adverse events).
The views expressed in this publication are those of the authors and do not necessarily reflect those of Mölnlycke Health Care.
Australian PITA Group meetings
A group of skin integrity and pressure injury clinical and academic experts were approached by Mölnlycke to form the Australian PITA Group. The group was formed in June 2021 and the first virtual advisory board meeting took place on 10th June 2021. Over a 12-month period, the group participated in a additional three online meetings, culminating in a final face-to-face meeting held in Sydney, Australia, in June 2022.
Throughout this series of formal advisory board meetings, with structured discussions moderated by Mölnlycke Health Care, the Australian PITA group collaborated to develop this ‘Quick Guide’. This guide was developed to assist clinicians responsible for managing pressure injuries across various clinical settings, including acute care, residential aged care, and community settings. Its purpose is to assist these clinicians in identifying and implementing evidence-based interventions that align with local standard care and current international guidelines.